Neuromuscular Electrical Stimulation (NMES) After ACL Reconstruction
Quadriceps weakness remains one of the most persistent impairments after anterior cruciate ligament reconstruction (ACLR). Despite structured rehabilitation, many patients fail to restore adequate strength, which can negatively affect function, return to sport, and long-term joint health.
A key contributor to this issue is arthrogenic muscle inhibition, where neural activation of the quadriceps is reduced following injury and surgery. In this context, neuromuscular electrical stimulation (NMES) has been proposed as a strategy to restore muscle activation and limit early atrophy.
This article reviews the rationale, evidence, and practical application of NMES in ACL rehabilitation.
Why consider NMES after ACLR?
Following ACL reconstruction, voluntary quadriceps activation is often impaired. This is not simply a matter of muscle weakness, but also an activation problem. NMES works by directly depolarizing motor neurons, producing involuntary muscle contractions. Therefore, NMES is primarily a tool for the early phase of rehabilitation, when activation deficits are most pronounced.
What does the evidence show?
A recent systematic review and meta-analysis of randomized controlled trials (2) found that
- NMES significantly improves quadriceps strength compared with standard rehabilitation alone
- These effects are present at both short-term and longer-term follow-ups
- Earlier use of NMES appears to produce greater improvements in strength recovery
This supports the idea that NMES is not a replacement for exercise, but a useful adjunct, particularly when voluntary activation is limited.
Earlier literature has also shown that NMES is superior to doing nothing, although voluntary exercise remains the cornerstone of strength development (3).
Clinical recommendations
The Aspetar clinical practice guideline on ACL rehabilitation (1) recommends the use of adjunct modalities such as NMES in the early phase, particularly when pain, swelling, and activation deficits limit exercise performance. There is also strong expert consensus supporting its use early after surgery to. Facilitate muscle activation, minimise disuse atrophy and support strength development alongside exercise
Practical application
When to use NMES
- In the early postoperative phase
- When quadriceps activation is poor
- As an adjunct to simple strengthening exercises (e.g. quad sets, straight leg raises)
- During early functional tasks
It should not replace progressive loading strategies later in rehabilitation.
Suggested parameters
- Current type: Biphasic / alternating
- Frequency: >50 Hz
- Pulse width: 250–400 μs
- Duty cycle:
- 10 seconds contraction
- 20–30 seconds rest
- 2–3 second ramp
- Intensity: Maximal tolerable (aim for a strong, visible contraction)
The key variable is intensity. Without sufficient intensity, the stimulus is unlikely to be meaningful.
Contraindications
NMES should not be used in the following situations:
- Cardiac pacemakers or electronic implants
- Pregnancy (abdomen/lower back)
- Known or suspected malignancy
- Active deep vein thrombosis
- Active bleeding or untreated hemorrhagic disorders
- Infected tissues or osteomyelitis
- Recently radiated tissue
- Chest in individuals with cardiac disease or arrhythmias
- Head/neck region in individuals with seizure disorders
NMES combined with blood flow restriction
An emerging area of interest is the combination of NMES with blood flow restriction (BFR). This approach aims to increase the overall training stimulus by combining mechanical activation (via NMES) with metabolic stress (via BFR). Experimental evidence shows that adding NMES to BFR can attenuate disuse muscle atrophy more effectively than BFR alone, particularly during periods of immobilisation . More recent systematic review (6) data suggest that this combined approach may promote greater hypertrophic adaptations compared to NMES or BFR in isolation, although current evidence remains limited and somewhat inconclusive. From a clinical perspective, this combination may be particularly relevant in the very early stages of rehabilitation, where voluntary loading is not yet possible. However, as with NMES alone, it should be viewed as a passive adjunct, not a replacement for progressive resistance training.
Key takeaways
- Quadriceps weakness after ACLR is partly neurological, not just muscular
- NMES can help overcome early activation deficits
- Evidence supports its use as an adjunct to rehabilitation
- The greatest benefit is seen when applied early and with sufficient intensity
- Exercise remains the foundation of ACL rehabilitation
CHATgpt created image based on this blogpost.

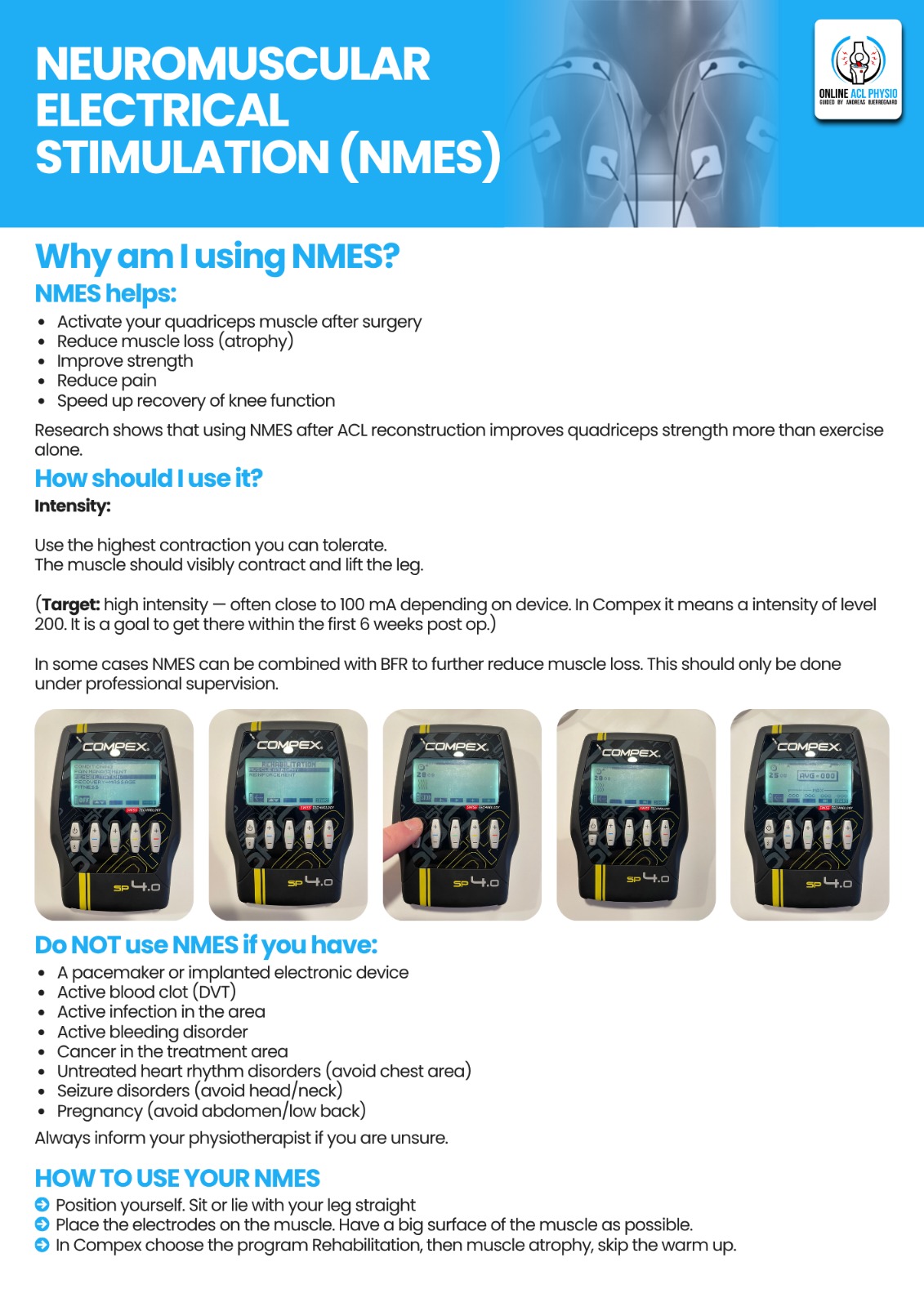
My guidelines to COMPEX for patients renting it as part of their rehab.
References
- Kotsifaki R, Korakakis V, King E, et al. Aspetar clinical practice guideline on rehabilitation after anterior cruciate ligament reconstruction. Br J Sports Med. 2023;57:500–514.
- Li Z, Jin L, Chen Z, et al. Effects of neuromuscular electrical stimulation on quadriceps femoris muscle strength and knee joint function in patients after ACL surgery: a systematic review and meta-analysis of randomized controlled trials. Orthop J Sports Med. 2025.
- Bax L, Staes F, Verhagen A. Does neuromuscular electrical stimulation strengthen the quadriceps femoris? A systematic review of randomized controlled trials. Sports Med. 2005;35(3):191–212.
- Natsume T, Ozaki H, Saito AI, Abe T, Naito H. Effects of Electrostimulation with Blood Flow Restriction on Muscle Size and Strength. Med Sci Sports Exerc. 2015
- Slysz JT, Boston M, King R, Pignanelli C, Power GA, Burr JF. Blood Flow Restriction Combined with Electrical Stimulation Attenuates Thigh Muscle Disuse Atrophy. Med Sci Sports Exerc. 2021
- Systematic review & meta-analysis (combined approach): Mangahas JK, Dalleck LC, Drummond C, et al. Effects of combined blood flow restriction and neuromuscular electrical stimulation on skeletal muscle hypertrophy in adults: a systematic review and meta-analysis. Scientific Reports. 2026.

